
Brand:
Economic Report of the President
Industry:
Health Care Policy
Business Type:
Government Report
Author:
Jonathan D. Keetcham
Summary:
Chapter 11 of the 2026 Economic Report of the President argues that decades of 'healthcare exceptionalism'—the belief that competition harms quality—have justified policies that distorted physician markets, disfavoring rural Americans and independent practices. The Trump Administration is reversing these distortions through the One Big Beautiful Bill Act, Medicare/Medicaid payment reforms, deregulation, and transparency enforcement—rebalancing supply, empowering independent physicians via site-neutral payments and reduced prior authorization, and leveraging telehealth and AI to reduce chronic disease burden.
Chapter 11 of the 2026 Economic Report of the President, prepared by the Council of Economic Advisers, challenges the persistent myth of 'healthcare exceptionalism'—the notion that competition among providers undermines quality and drives waste.
Decades of empirical research show the opposite: competition lowers prices, improves access, and enhances quality. Yet misguided regulations and flawed payment systems have distorted physician markets, creating long wait times (31 days average for new patient visits in 2025), systematic undersupply in rural areas, and consolidation that favors hospital-employed over independent physicians.
The chapter details how the Trump Administration is dismantling these distortions through the OBBBA's $50 billion Rural Health Transformation Program, HPSA designation reforms, site-neutral Medicare payments, Medicaid SDP caps, prior authorization streamlining, enhanced price transparency, telehealth expansion, and AI adoption—working to enable faster, more affordable, and higher-quality physician services.
Chapter 11
Making America Healthy by Unleashing Competition in Physicians’ Markets
Healthcare reforms in 2025 have confronted one of the most damaging myths in U.S. health policy—“healthcare exceptionalism,” the notion that competition between healthcare providers undermines quality and drives waste. Decades of evidence demonstrate the opposite: competition lowers prices, improves access, and enhances quality. Yet misguided regulations and flawed payment systems have distorted physicians’ markets in ways that have disfavored rural Americans and independent physicians. This chapter details how the Trump Administration is dismantling these distortions through the One Big Beautiful Bill Act (OBBBA), Medicare and Medicaid payment reforms, deregulatory initiatives, and enforcement of transparency rules.1 It highlights how eliminating existing biases will rebalance physician supply between urban and rural areas; how site-neutral payments, reduced prior authorization, and streamlined reporting will empower independent practices; and how prevention-focused initiatives, telehealth expansion, and artificial intelligence are tackling the chronic disease burden that drives demand. Together, these reforms will enable faster, more affordable, and higher-quality physician services for Americans.
Like many sectors of the U.S. economy, special interest groups in healthcare aim to shape legislation and regulations in the service of their own financial gains. This dysfunction has been justified by the persistent
idea that somehow healthcare is “different” from other industries in ways that make competition potentially harmful. A particular concern is labeled “supplier-induced demand,” an application of Say’s law, which holds that greater Information in this chapter is up to date as of November 20, 2025. competition among hospitals or physicians will promote greater provision of low-value, low-quality care. These concerns have provided some of the justification for decades of piecemeal industrial-planning interventions by Federal and State governments alike.
However, decades of empirical research belie the falsehood of this jus-
tification. In insurance markets, competition lowers premiums and promotes diverse plan designs in ways that increase enrollment (Dunn 2009). For hospitals, research finds that patients are disproportionately drawn to higher-quality hospitals, and that differences between hospitals in productivity measures are at least as small as differences between manufacturing firms (Chandra et al. 2016a, 2016b). These findings that quality is rewarded in hospital markets led the authors to conclude, “contrary to the long tradition of ‘healthcare exceptionalism’ in health economics, the healthcare sector may have more in common with ‘traditional’ sectors subject to standard market forces than is often assumed” (p. 102). Research has also found lower prices from competition between pharmaceuticals and durable medical equipment, particularly when competition is not hindered by regulations (Danzon and Chao 2000; Ding, Duggan, and Starc 2025).
Likewise, competition between physicians has benefited Americans.
Studies report 20 percent lower prices paid by commercially insured patients in the least concentrated markets compared with the most, with a 10 percent decrease in physicians’ market concentration decreasing prices by 0.5-1 percent (Clemens and Gottlieb 2017; Dunn and Shapiro 2014). The benefits of competition are particularly evident among services where third-party payment is relatively rare or when patients are responsible for the differences in cost between providers (Perry 2022; Robinson and Brown 2013). Entry of competing physicians has been shown to improve access and quality as well. Specifically, research on the expansion of residency training programs in obstetrics and emergency medicine found that they led to improved access to care overall and to higher-quality care specifically, without increasing the use of more costly, intensive treatments (Rabideau, Richards, and Whaley 2024).
These findings of greater competition promoting access and quality
provides additional evidence against the view that an increased supply of physicians’ services promotes supplier-induced demand. This builds on decades-old research showing that the methodology used in the original studies supporting the “supplier-induced demand” hypothesis also leads to the implausible conclusion that more obstetricians in a market cause more babies to be born (Dranove and Wehner 1994). Despite this evidence, the false but persistent view of healthcare exceptionalism has been used to justify policies that have harmed Americans by hindering competition among physicians. The policies include regulations and payment programs that have created barriers to entry and incentives for vertical and horizontal consolidation among physicians.
The U.S. healthcare system presents evidence of the problem, including:
Figure 11-1. Average Waiting Time for a New Patient Visit, by Specialty and Year
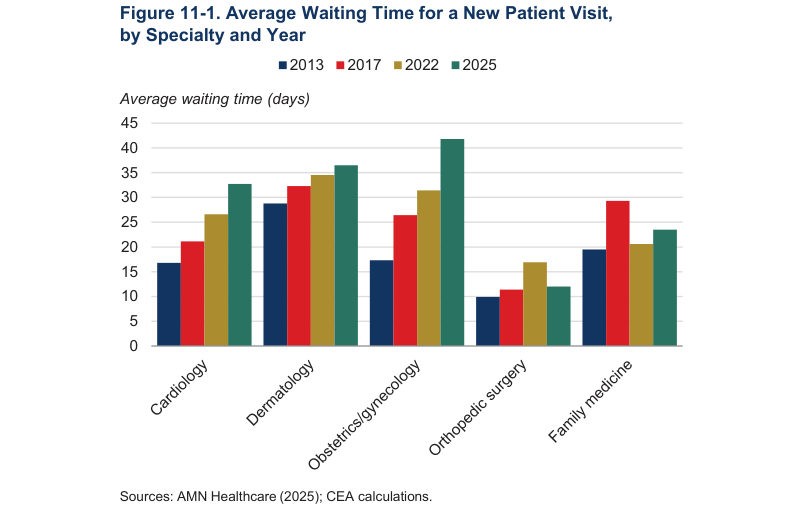
Sources: AMN Healthcare (2025); CEA calculations.
Figure 11-2. Average Number of Physicians per 10,000 Population by Type and Location
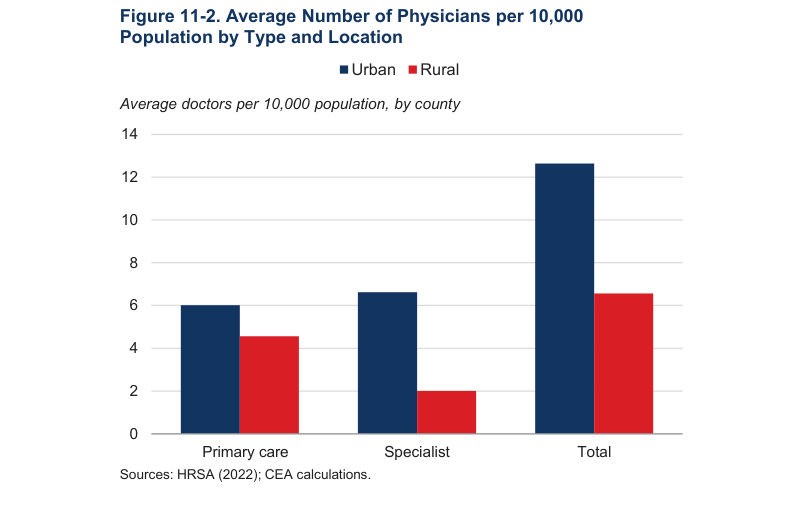
Sources: HRSA (2022); CEA calculations.
Figure 11-3. County-Level Distribution of the Number of Physicians per 10,000 Population by Type and Location
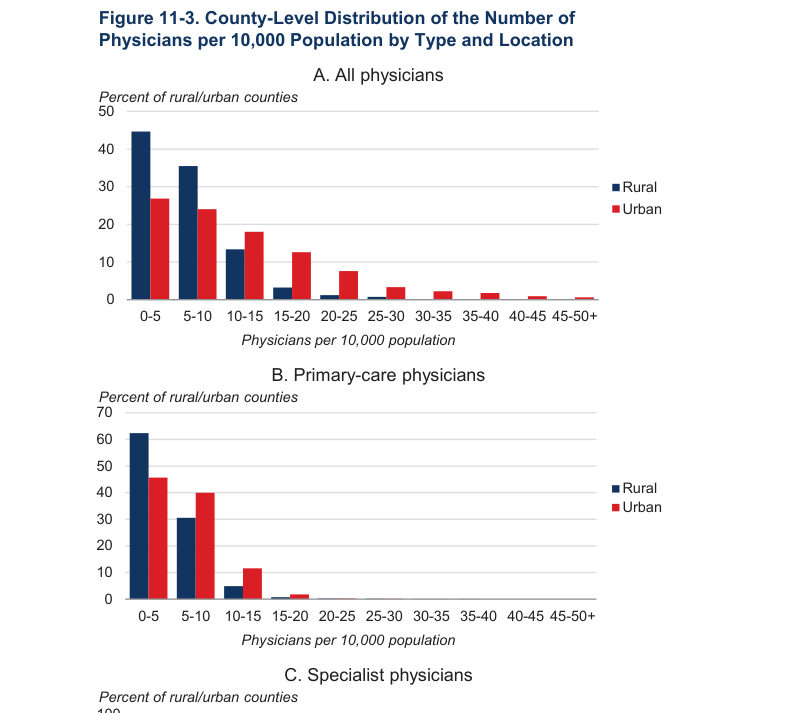
Source: AMN Healthcare Survey (2025); CEA calculations.
Long waiting times for visits, with a 2025 survey reporting an average of 31 days for new patient appointments across 15 major U.S. cities, up 19 percent from 2022 and 48 percent from 2004 (AMN Healthcare 2025) (figure 11-1).
High internal rates of return to medical specialization that have persisted for decades, partly due to limited residency spots controlled by specialties themselves (Nicholson 2003; Bhattacharya 2005).
Rapid growth of other suppliers seeking to address the unmet demand. This includes entry of retail clinics and urgent care centers and growth of physician extenders that is forecasted to continue (RAND 2016; Fortune Business Insights 2025; Bureau of Labor Statistics 2025).
Fewer physicians per capita, an often-used proxy measure for undersupply. As shown in figures 11-2 and 11-3, these differences are systematic, and larger for specialist physicians. For example, nearly half (48.6 percent) of urban counties have 10 or more physicians per 10,000 population, versus 19 percent of rural counties. For specialists, 20 percent of urban counties have 10 or more per 10,000 population, while this is true for only 1.5 percent of rural counties.
This chapter discusses steps that the Trump Administration has already
taken to correct specific government-driven supply-side distortions away from efficient, market-driven outcomes and to alleviate demand by reducing the burden of chronic illness and leveraging new technology.
Addressing Biases Against Rural Americans
Historically, Federal programs have exacerbated the misallocation of existing physician supply between geographic areas in ways that have disfavored rural areas. In response, the One Big Beautiful Bill Act established the Rural Health Transformation Program, which provides $50 billion over five years (2026–30) to States via the Centers for Medicare & Medicaid Services (CMS) for rural health improvements (H.R. 1833; see U.S. Congress 2025). This includes grants and technical assistance to rural healthcare providers, including funding for telehealth infrastructure and workforce development. Notably, two of the stated aims of the program are to attract and retain a highly skilled healthcare workforce by strengthening recruitment and retention of healthcare providers in rural communities (CMS 2025g). To reward and promote competition in physician markets specifically, the grant applications are scored based on whether State-level policies minimize Certificate-of-Need laws that prohibit entry by healthcare providers; broaden scope-of-practice rules for providers of primary care, and recognize medical and nursing licenses granted by other States (CMS 2025g).
Additional long-standing biases against rural areas are being addressed
through ongoing reforms to the Health Professional Shortage Areas (HPSAs) defined by the Health Resources and Services Administration (HRSA 2025). The reforms are updating HPSA definitions to replace decades-old definitions that fail to incorporate current supply of primary care in ways that bias against rural areas (Paragon Health Institute 2024). As a result, many areas with an HPSA status have greater availability of physicians than do areas without an HPSA designation. HRSA is using updated methodology and data to improve the accuracy of the HPSA designation and government resources along with it. These reforms will correct existing government-created problems with the allocation of physicians because over 30 Federal programs are tied to HPSA designation: it determines eligibility for incentives such as Medicare’s 10 percent bonus payments for physicians serving in HPSAs, J-1 visa waivers for international medical graduates to practice in the United States without returning home for two years, and enhanced reimbursement rates under Medicaid or the Federally Qualified Health Center program (Government of the District of Columbia, Department of Health, n,d.).
Critically, HPSA scores prioritize funding and placements in the National
Health Service Corps (NHSC) Loan Repayment Program (LRP) (NHSC n.d.). This program ties loan forgiveness for primary care physicians and nurse practitioners to serving in locations that receive high scores in the HPSA identification methodology. A 2021 GAO report found that flawed designations have given financial rewards to physicians for locating in relatively well-supplied metropolitan areas, diverting physicians from truly rural or isolated spots where shortages are acute.
Furthermore, the program’s funding priorities, which favor high-score
HPSAs for awards up to $100,000 over three years, have been overallocated to States that spend large amounts to game the system (e.g., Northeastern urban areas), disadvantaging rural areas relative to the allocation that would result from greater market signals without these government-designed distortions (NHSC 2021). By fixing the HPSA designations, the reforms ensure that resources go where they are needed most, improving rural access, reducing costs through efficient allocation, and enhancing quality by attracting dedicated providers.
Addressing Distortions Caused by Regulations and Flawed Payment Programs
Nearly 80 percent of physicians are employed by hospitals, health systems, or corporations in 2024 (Condon 2024). This is at an all-time high, after years of a shift away from independent practices, which was driven in part by rising regulatory and administrative burdens and government-designed financial incentives.
Addressing the Regulatory and Administrative Burden
Regulations create high fixed costs through compliance requirements, reporting, and administrative burdens that disfavor smaller firms, such as independent physicians’ practices and practices located in rural markets. High fixed costs promote consolidation (horizontal mergers among practices) and vertical integration (e.g., physicians joining larger health systems or hospitals). In fact, between 2012 and 2022, the share of physicians in practices with 50 or more doctors rose from 12.2 to 18.3 percent (Kane 2023). Vertical integration has also surged, with hospital-employed physicians increasing from 23.4 percent in 2012 to 34.5 percent by 2024 (Advisory Board 2025).
These trends are largely attributed to rising regulatory burdens and
increased administrative costs (American Hospital Association 2025). A 2016 study estimated that physicians spend about 15.1 hours a week on paperwork for quality reporting alone, costing roughly $40,000 per physician annually in lost productivity (Casalino et al. 2016). These costs disproportionately burden small practices. A Federal Trade Commission (FTC) workshop in 2018 highlighted how regulatory complexity drives physicians to affiliate with hospitals, as larger entities can better absorb fixed costs for information technology infrastructure and legal expertise (Kane 2023). This consolidation led to higher prices paid by Americans for the same services, and increased spending by Medicare (Capps, Dranove, and Ody 2018; Cooper et al. 2025; U.S. Government Accountability Office 2025).
The Trump Administration is actively working to reduce administrative
burdens, for example, through Executive Order 14192 (Federal Register 2025c). Within healthcare specifically, the Department of Health and Human Services (HHS) has secured a commitment from private insurers to reduce unnecessarily burdensome prior authorizations that create compliance costs for physicians (U.S. Department of Health and Human Services 2025). The Department of Justice issued a Request for Information (RFI) with an emphasis on physicians specifically as part of efforts guided by its anticompetitive regulations task force (Antitrust Division 2025). CMS also issued a Medicare Regulatory Relief RFI in July 2025 to solicit public feedback on ways to “streamline regulations and reduce administrative burdens on providers” based on the recognition that “healthcare providers serving Medicare beneficiaries face numerous regulatory requirements” (CMS 2025f). Finally, the FTC issued warning letters to large healthcare employers indicating that their noncompete clauses and other restrictive covenants with employed physicians would be scrutinized, particularly in rural areas (McDermott Will & Schulte 2025).
Addressing Distortions Caused by Physicians’ Payment Methods
Consolidation has also been fueled by distortions in policies that guide how Federal programs pay for physicians’ services. The Trump Administration is actively working to correct prior distortions and improve efficiency through three channels.
The first channel is Medicaid reform in the OBBBA. Before the OBBBA,
State-directed payments (SDPs) in Medicaid managed care allowed States to direct the amounts health plans pay providers, which in some cases disfavored independent physicians’ practices. Specifically, States used SDPs to increase Medicaid payments to hospitals above what their Medicaid programs would have paid otherwise, and these adjustments exceeded those that States implemented for physicians.
In 2024, SDP spending was about $110 billion across 302 arrangements in
40 States, nearly 60 percent above the amount approved just the year before. This is partly driven by the fact that rules allowed States to leverage SDPs to pay hospitals at rates up to the levels paid by commercial insurers, which far exceed rates paid by Medicaid and even Medicare (Federal Register 2024; Congressional Budget Office 2022). In addition to exacerbating a rapid rise in projected Medicaid spending, SDPs are disproportionately concentrated on hospitals (Congressional Budget Office 2024). Of the programs in 2024, 53 percent were directed to hospitals versus just 11 percent to physicians, with the remainder going to other facilities such as nursing homes. Among the 29 arrangements with additional spending estimated to be above $1 billion per year, 24 were targeted to hospitals (MACPAC 2024). In California, for example, independent physicians are not eligible for the six hospital SDP programs that allocate about $12 billion annually in additional payments through MediCal (California Department of Finance). These adjustments boosted MediCal payments to hospitals. In contrast, in 2024 California did not have any SDPs designed to increase payments to independent physicians’ practices above the State’s Medicaid payment levels.
The OBBBA addresses these imbalances by capping SDPs at 100 percent
of Medicare rates for Medicaid expansion States (110 percent for nonexpansion States), phasing down higher existing payments by 10 percentage points annually starting in 2027. This corrects the long-standing practice of States directing disproportionate shares of additional Medicaid spending through SDPs to hospitals rather than physicians’ practices.
The second channel is payment rules in traditional Medicare. The
Administration has taken a number of steps in 2025 to correct distortions created by Medicare payment rules.
In July 2025, CMS released the Calendar Year (CY) 2026 Hospital
Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) proposed rule, which expands site-neutral payment policies to include drug administration services (e.g., infusions and injections) furnished at all off-campus provider-based departments of hospitals (excluding rural sole community hospitals). Under this proposal, these services would be reimbursed at the lower Physician Fee Schedule (PFS) rate rather than the higher OPPS rate. By removing the increase in Medicare payment for administering these services at hospital-owned physicians’ practices, this rule will reduce the financial incentives for hospitals to acquire independent practices.
The rule also proposes repealing the Inpatient-Only list over three years
and expanding the ASC Covered Procedures List, allowing more procedures to shift to lower-cost outpatient or ASC settings. This further promotes site neutrality and levels the playing field between independent physicians’ practices and those controlled by hospital systems (CMS 2025b).
The CY 2026 PFS Proposed Rule, also released in July 2025, complements
this by updating practice expense calculations by site-of-service to better recognize costs for independent physicians compared with hospital-employed ones, moving toward greater payment equity and reducing market distortions that fuel consolidation (CMS n.d., b; 2025c).
The third channel includes innovative methods and flexibility through
the Center for Medicare & Medicaid Innovation (CMMI). CMMI, which was created to test innovative payment and delivery models, has proposed in 2025 the Ambulatory Specialty Model (ASM). ASM mandates participation for specialists in 240 areas treating conditions like heart failure and low back pain, applying payment adjustments (plus or minus 9-12 percent by 2033) based on cost and quality performance across all services. The model supports independent physicians’ efforts to provide value-based arrangements without requiring hospital integration (CMS 2025a).
Meeting America’s Needs with Transparency, Technology, and Scientific Transformation
In 2025, Federal price transparency requirements under the Transparency in Coverage (TiC) and Hospital Price Transparency rules were enhanced after the issuing of Executive Order 14221, which emphasized accurate pricing data (Federal Register 2025a). For TiC, the Administration updated technical specifications for greater usability to be implemented by February 2026 (U.S. Department of Labor 2025). The Hospital Price Transparency rule revisions in 2025 now mandate hospitals to report payer-specific negotiated rates as actual dollar amounts, replacing ambiguity and a lack of standardization (CMS 2025d). By making prices visible, these rules empower patients to choose lowercost providers, fostering competition that drives down costs and improves access to affordable options. In addition to driving price competition directly, it can also improve the allocation of physicians across geographical areas and service types by indicating where undersupply is exacerbating high prices. Finally, transparency discourages consolidation of physicians’ practices and vertical integration with hospitals by empowering patients and payers to seek lower-cost independent providers.
The Trump Administration has also taken steps to improve access and
lower costs for fertility care, specifically in three areas. First, the Administration has proposed requirements for providers to report more transparent, uniform information about their prices and clinical outcomes to facilitate comparisons and consumer decision-making. Second, efforts are being made to expand access to physicians who are willing and able to provide fertility services, including for in vitro fertilization, for example, by removing some of the barriers created by accrediting bodies. Third is the recognition of fertility services as an “excepted benefit,” allowing stand-alone insurance plans that can help people to navigate their care. Collectively, these efforts equip Americans with better information, better access, and navigation support to overcome the challenges created by the relatively small set of clinics and subspecialists and limited entry of new providers under the status quo (Centers for Disease Control and Prevention 2024; National Resident Matching Program 2025).
In June 2025, HHS and CMS also struck a voluntary agreement to reduce
and streamline prior authorizations involving major health insurers (e.g., UnitedHealth, CVS Health / Aetna, Humana). Commitments include reducing the number of claims requiring prior authorizations, implementing standardized electronic processes of requests, and expanding real time responses for requests (United States Department of Health and Human Services 2025). This will cut the administrative burdens faced by physicians and aligns with CMS’s goals to improve efficiency and patient access (U.S. Department of Health and Human Services 2025; AHIP 2025). For Americans, this means faster approvals for needed care, reducing delays in access, lowering administrative costs passed to patients, and allowing physicians to focus on high-quality treatment efforts to prevent chronic diseases, particularly among children, by developing prevention-focused systems (White House 2025b). By tackling the root causes of chronic illnesses, MAHA efforts will reduce demand for physicians’ services, easing shortages, lowering overall healthcare costs, and improving population health.
The proposed change to the 2026 Medicare physician fee schedule also
prioritizes disease prevention, including with digital health technology (i.e., telehealth). The CY 2026 PFS expands telehealth flexibilities, such as lifting frequency limits and adding new codes for virtual care, enhancing access to preventive services, particularly in rural areas (Federal Register 2025b). The Medicare Diabetes Prevention Program revisions to 2025 allow fully online care now through December 2029, expanding virtual delivery without in-person requirements to broaden access and manage and prevent chronic conditions (CMS 2025e). These changes improve access via remote options, reduce costs by preventing expensive treatments, and enhance quality through early intervention.
The Trump Administration has positioned the United States to lead on
the use of digital tools to meet Americans’ needs for care, including artificial intelligence specifically (CMS 2025h; White House 2025a). These tools will be both physician-facing—such as diagnostic aids to promote individualized, evidence-based care—and patient-facing, such as those that can help manage chronic conditions and leverage price transparency data. These steps have paved the way for innovators to meet Americans’ needs for faster diagnoses, more efficient resource use, and tailored treatments.
Conclusion
“Healthcare exceptionalism”—the idea that competition in healthcare is harmful—has been one of the most persistent and pernicious ideas in the U.S. healthcare system. As a result of this view, and the policies that it has propped up over decades, one way that healthcare has been “exceptional” is in the degree to which government has hindered competition and caused distortions, moving the industry away from efficient, market-based outcomes. The Trump Administration has already taken a number of steps to correct the distortions caused by prior government policies that have disfavored rural Americans and independent physicians. By addressing both supply-side and demand-side causes of past challenges, the Administration is proactively working to equip the U.S. healthcare system to meet the Nation’s needs, lower prices, and improve access and quality.

